
SNHL Explained: Causes, Signs, and Modern Treatment Options for Nerve Deafness
1.5 billion people worldwide live with hearing loss. Yet the average person waits 7 to 10 years after noticing the first signs before seeking help.
That gap isn’t just frustrating – it’s dangerous. Because what most people don’t know is that untreated hearing loss is one of the most significant modifiable risk factors for dementia. Every year of delay isn’t just a year of missed conversations. It may be a year your brain can’t afford to lose.
- Written by: karishma Rautela
- Review by: Mahipal Dosad

What Is Sensorineural Hearing Loss?
Sensorineural hearing loss is the most common type of permanent hearing impairment. It occurs when there is damage to the inner ear (cochlea) or the auditory nerve that carries sound signals from the ear to the brain.

Unlike conductive hearing loss – which involves a blockage or mechanical problem in the outer or middle ear (think earwax buildup, fluid from a cold, or a perforated eardrum) – SNHL is a nerve-level problem. The sound reaches the inner ear, but the hair cells or neural pathways that process it are damaged or destroyed.
Mixed hearing loss, as the name suggests, involves elements of both.
The practical difference matters: Conductive hearing loss is often temporary and treatable. Sensorineural hearing loss is usually permanent – though it is absolutely manageable.
Common Causes of Sensorineural Hearing Loss

SNHL doesn’t have a single origin story. It builds from a surprisingly wide range of causes:
Aging (Presbycusis)
The most prevalent cause. The tiny hair cells inside the cochlea don’t regenerate in humans – so decades of sound exposure gradually erode them. High-frequency hearing typically fades first, which is why older adults often struggle to follow fast conversation even when volume isn’t an issue.
Noise Exposure
Prolonged exposure to loud environments – construction sites, concerts, earbuds at high volume – is the leading preventable cause of SNHL, particularly in younger adults.
Systemic Health Conditions
This is where many people are surprised. SNHL doesn’t stay in the ear – it often reflects what’s happening throughout the body:
- Diabetes and pre-diabetes: Elevated blood sugar damages the blood vessels supplying the cochlea. Research consistently links both Type 2 diabetes and pre-diabetic states to increased tinnitus and early hearing decline.
- Hypertension (high blood pressure): Reduced blood flow to the inner ear can accelerate cochlear cell death. Multiple studies confirm a significant link between uncontrolled hypertension and hearing loss – and in some cases, managing blood pressure has helped slow further decline.
- Kidney disease: The kidneys and inner ear share remarkably similar microstructures. Chronic kidney disease disrupts electrolyte balance and blood filtration in ways that can directly affect hearing and contribute to tinnitus and vertigo.
- Stroke: A stroke affecting the auditory cortex or blood supply to the inner ear can cause sudden SNHL. This is sometimes called an “ear stroke” (sudden sensorineural hearing loss or SSNHL) – a medical emergency requiring treatment within 72 hours.
- Chemotherapy: Certain chemotherapy drugs, particularly cisplatin, are ototoxic – meaning they are toxic to the auditory system. Tinnitus during or after chemo is common, and permanent hearing damage is a documented side effect.
Infections and Illness
Viral infections – including severe colds and flu – can cause temporary hearing reduction due to fluid and inflammation. In rarer cases, infections like meningitis can cause permanent cochlear damage.
Auditory Processing Disorder (APD)
Often confused with SNHL, auditory processing disorder (APD) is a different but related condition. People with APD can physically hear sounds adequately, but their brain struggles to correctly interpret what it hears – especially in noisy environments. APD is particularly common in children and adults with attention difficulties. Diagnosis requires specialized central auditory processing testing, separate from a standard audiogram.
How Is Sensorineural Hearing Loss Diagnosed?
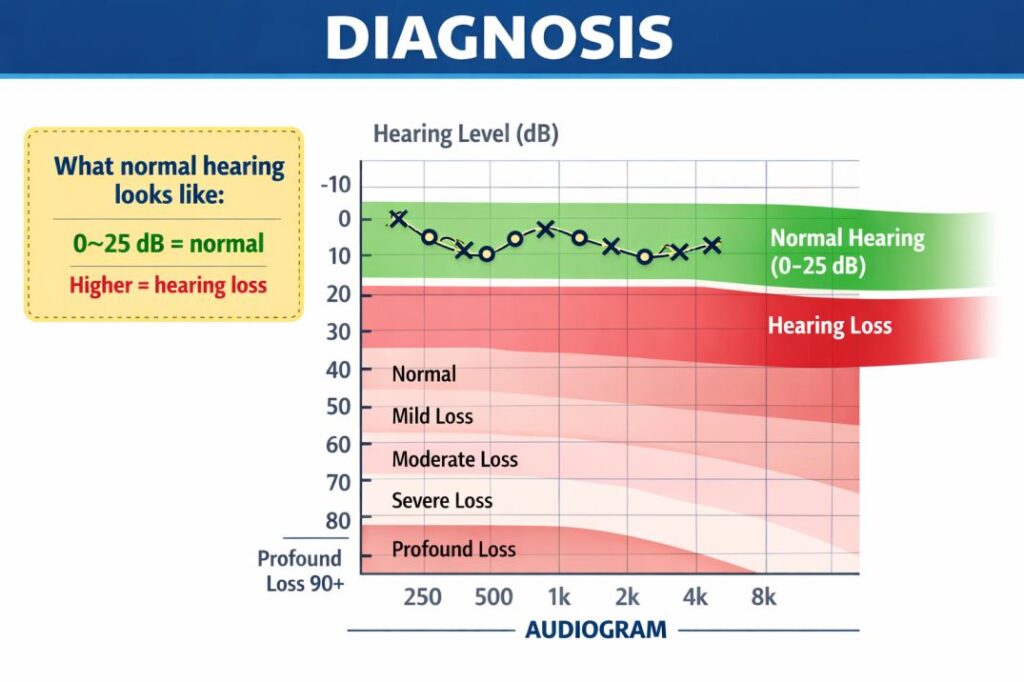
dDiagnosis begins with an audiogram – a standardized hearing test that maps how well you hear tones across different frequencies, measured in decibels hearing level (dB HL). A normal hearing audiogram typically shows responses at or better than 25 dB HL across frequencies.
SNHL shows up as reduced sensitivity particularly at higher frequencies, creating a characteristic sloping pattern on the audiogram. Severity is classified as:
- Mild SNHL: 26–40 dB HL
- Moderate SNHL: 41–55 dB HL
- Severe SNHL: 71–90 dB HL
- Profound SNHL: 91+ dB HL
For suspected retrocochlear hearing loss (damage along the auditory nerve rather than the cochlea itself), additional tests like ABR (auditory brainstem response) may be ordered.
Can Sensorineural Hearing Loss Be Reversed?

This is the question nearly everyone asks – and the honest answer is: not yet, but science is moving fast.
Currently, damaged cochlear hair cells cannot be regenerated in adults. However, several promising treatment directions are actively in clinical development:
- Gene therapy targeting hair cell regeneration has shown remarkable results in early trials
- Stem cell research is exploring cochlear repopulation
- Drug therapies aimed at protecting surviving hair cells from further damage
For most people today, the primary treatment remains hearing aids designed specifically for sensorineural loss – which amplify and shape sound to compensate for the damaged frequencies. Severe-to-profound SNHL may benefit from cochlear implants, which bypass the damaged cochlea entirely and directly stimulate the auditory nerve.
Living With SNHL: Where Technology Helps Right Now
While science works toward a cure, practical tools are making a real difference in daily life – and live transcription apps are among the most impactful.
Apps that convert spoken words to on-screen text in real time help SNHL patients follow conversations in settings where hearing aids alone aren’t enough: crowded meetings, lectures, medical appointments, or one-on-one conversations in noisy environments. Many users report that pairing their hearing aids with a live transcription app dramatically reduces the cognitive fatigue of “effortful listening” – the exhausting mental work of reconstructing speech from partial auditory input.
Beyond transcription, captioned telephone services, loop systems in public spaces, and Bluetooth-enabled hearing aid streaming are all lowering the daily barriers that SNHL creates.
The Hearing Loss–Dementia Connection
One of the most significant findings in hearing research over the past decade is the strong link between untreated hearing loss and cognitive decline. Multiple large-scale studies have found that people with moderate hearing loss have up to three times the risk of developing dementia compared to those with normal hearing.
The leading explanation: when the brain works overtime to interpret degraded auditory signals, cognitive resources are diverted from memory and reasoning. Social withdrawal caused by hearing difficulty may further accelerate decline.
The takeaway is urgent – treating hearing loss early isn’t just about hearing better. It may protect your brain.
Conclusion: What You Should Do Next
Sensorineural hearing loss is common, complex, and still underdiagnosed – partly because it develops gradually and partly because people adapt to it so quietly that years pass before they seek help.
Key takeaways:
- SNHL is nerve-level hearing loss, distinct from conductive or mixed types
- It is linked to diabetes, hypertension, kidney disease, stroke, and chemotherapy – making overall health management directly relevant to your hearing
- It is currently not reversible, but highly treatable with hearing aids, implants, and assistive technology
- Live transcription apps offer immediate, practical support for daily communication
- Early treatment matters – for quality of life and long-term cognitive health
If you’ve been wondering whether your hearing has changed, trust that instinct. A proper audiometric screening is the first step toward answers.
Frequently Asked Questions
What is the most common cause of sensorineural hearing loss in adults?
Aging (presbycusis) and prolonged noise exposure are the two leading causes. Both progressively damage cochlear hair cells, which do not regenerate naturally.
Can high blood pressure cause sensorineural hearing loss?
Yes. Chronic hypertension reduces blood flow to the cochlea, which can accelerate hair cell damage. Managing blood pressure may help slow further progression.
How is SNHL different from auditory processing disorder (APD)?
SNHL is a problem with hearing the sound itself – the ear or auditory nerve is damaged. APD is a brain processing issue – the sound arrives correctly but the brain struggles to interpret it accurately.
Does chemotherapy always cause hearing loss?
Not always, but certain chemotherapy drugs (particularly cisplatin) are ototoxic and carry a significant risk of causing tinnitus and permanent hearing damage. Monitoring is essential during treatment.
Can live transcription apps help people with sensorineural hearing loss?
Yes – live transcription apps convert speech to on-screen text in real time, helping SNHL patients follow conversations in noisy or fast-paced environments where hearing aids may not be sufficient on their own.
Is there a link between kidney disease and hearing loss?
Yes. The inner ear and kidneys share similar structural proteins and filtration mechanisms. Chronic kidney disease can disrupt inner ear function, contributing to both hearing loss and tinnitus.



